Knowledge the Enterprise Resource Planning System in Hospitals and Health Care Centers in Basrah
Nael Jaafar Ali1 , Zinah abdulsttar Abdullah2 luay abdulwahid shiha3
1instructor of basic science college of nursing – university of Basrah
2Ass. instructor of basic science college of nursing – university of Basrah
Zinah.abdulsttar@uobasrah.edu.iq
3 Ass.prof. department of basic science – college of nursing – university of Basrah
Luay.abdulwahid@uobasrah.edu.iq
HNSJ, 2024, 5(12); https://doi.org/10.53796/hnsj512/16
Published at 01/12/2024 Accepted at 05/11/2024
Citation Methods
Abstract
Enterprise resource planning (ERP) is an integrated system for managing the administrative, financial and medical aspects of hospitals and health care institutions. The system aims to organize the work in the hospital to allow access to the patient’s data and follow-up while he is in the hospital, to organize the provision of service to the patient in an optimal manner and in the fastest time, to organize appropriate treatment programs for each case, and to facilitate the doctor’s work through medical registration of the patient’s condition (complaints and symptoms – examinations, analyzes and radiology – Operations – Diagnostics – Doctors’ orders and follow-up on their implementation – Follow up the progress of the patient’s condition – Medications and medical recommendations), which facilitates the follow-up of the patient’s health development and ensures accuracy and speed of performance.. Problem of the project: What is the level of knowledge of health personnel about ERP? What is the relationship between demographic variables and health personnel’s knowledge of ERP?
Objective: the study aims to increase revenue, improve performance, reduce risk, providing a classification of the ERP integration concept in a healthcare Organization. Methodology:
This study included a sample of health staff members numbering (71), and the study uses a questionnaire that includes (24) items to verify the sample’s knowledge about the enterprise resource planning system. For the purpose of data analysis, the arithmetic mean, standard deviation, percentage, and a sample dependent test were Chi-square.
the majority of health cadres (59.2%) are
female, and with regard to the educational level, the majority (35.2%) of the sample was (diploma). Years of service The majority (35.2%) of the sample (10-6) years. Regarding the housing environment, the majority were city dwellers. Table (4-2) indicates that health personnel have good knowledge of general information about the enterprise resource planning system. Table (3-6) indicates that there is no relationship between the knowledge of health staff members and demographic information about the ERP system and the impact of this.
The study shows that percentage of successful knowledge about ERP is 77.5% while the proportion of Poor knowledge 21.1%.
Key Words: study, financial and medical, design System in Hospitals .
Introduction :
ERP’s complexity and high expenses Numerous businesses are being forced to reassess their new ideas due to implementation issues. With respect to this business system [1]. on assisting people in making health- promoting or -protecting behavioral choices: as an example, Smoking, eating well, exercising, and decreasing stress are all good things to do. Despite the fact that ERP programs are the well-structured, dependable information technology (IT) backbones of Fortune 500 firms throughout the world [2]. ERP improves the efficiency of health-care services, reduces patient wait times in emergency rooms, and streamlines service work. By using ERP, the stations can provide better value for their purchases at pharmacies, and the pharmacies can provide better value for their purchases. The organization enhances the efficiency of existing business processes, reduces receivable days, and improves customer service. Credit returns are increased, as well as back-end efficiency [3]. Health care, particularly hospitals, is viewed as a new and expanding industry by major ERP system providers such as SAP and Oracle. As a result, specialized applications such as care management and patient logistics have emerged. The ERP system has been designed to fulfill the needs of hospital finance and general management. in regard to the hospital setting Hospitals differ from other types of facilities for a variety of reasons. These factors may have an impact on the deployment and use of an ERP in this industry ,setting. First, hospitals have a wide range of goals, including treating and caring for patients as well as teaching and educating future doctors and nurses. Because of the diversity of the hospital workforce, implementing [3].
Using an ERP system necessitates the participation of a wide number of people. a wide range of experts, including doctors, nurses, and other medical professional’s groups that give non-medical services, such as hospital managers, to laboratory assistants as well as IT departments [4].proposed three possible rationalities in this context. Technical, managerial, and medical issues all have the potential to collide. The term “technical rationality” refers to the ability to make decisions based IT experts and IT vendors who share a technical viewpoint on which to make their decisions. designs of systems Managerial rationality refers to hospital executives who make decisions based on legal, financial, and control considerations. ERP, in its most basic description, is an enterprise- wide information system that combines and controls all of a company’s business processes [4]. ERP stands for “a packaged business software system that allows a corporation to manage its operations.” the efficient and effective use of resources (materials, human resources, financial resources, and so on) by a company. delivering a comprehensive, integrated solution for the information-processing demands of the organization.” This If well-implemented, software permits the integration of all functional information flows. throughout the company into a single package with a centralized database as a result, it enables quick and immediate access to inventory, product, and customer information, and information about the past [5]. Physicians require immediate access to patient information and data kept in hospital and clinical information systems. For healthcare organizations, efficient patient care delivery by physicians and clinicians is a must. The research demonstrates how ERP deployment affects data. stakeholders such as management, monitoring, data retrieval, and data storage administrators and physicians. In terms of managing medical services or healthcare monitoring difficulties, management impact, expenses, and increasing the quality of care, ERP has a lot to consider [6]. We can cut patient wait times, credit refunds, and other costs by deploying ERP. Boost the efficiency of the backend.
This work is based on exploratory research, which entails examining historical situations involving county hospitals and pharmaceutical companies, in which ERP had a key role in improving overall efficiency. ERP are particularly positioned to record, store, analyze, and convey timely information to decision makers for better healthcare coordination at both the individual and population levels, in addition to their inherent function in clinical and diagnostics equipment. For Data mining and decision assistance capabilities, for example, might indicate potential negative outcomes for a single patient while also contributing to the overall health of the population by offering insights investigation into the origins of disease complications Recent reports emphasize the seriousness of adverse effects. clinics, dispensaries, and hospitals, as well as the risks that such incidents bring to individuals and the general public [7]. The word Big Data is generally synonymous with exorbitant volumes of data. This idea must be put aside because Big Data is not only targeted at a massive scale, it rather includes both the quantity and range of data and the speed and efficiency of entry. The process has now been moved to contact, to get the most value from the information produced minute by minute [8].
Methodology :
Validity of the Study Instrument
The validity has been determined for the evaluation of the tool through a penal of eight experts, faculty members from College of Nursing
/ University of Basra; who have necessary experience that qualify them to exam the content of the questionnaire. Those experts were request to review the instruments for content, clarity, relevancy, and competence; some items were accepted and others were added after a face-to-face discussion with each expert and subsequently the instrument was represent valid after getting all the comments and recommendations in consideration.
Evaluation of Questionnaires Score as following table.
|
Table(3-1): three point Likert Scale |
|
|
Level |
Ass. |
|
0 – 0.33 |
Poor |
|
0.34 – 0.67 |
Moderate |
|
0.68 – 1 |
Good |
Table (3-1) shows three level of Likert scale; the first level is poor was (0 – 0.33), the second level is moderate was (0.34 – 0.67), and the third level is good was (0.68 – 1) .
Results of the Study :
This chapter deals with analysis of the data through statistical procedure. N = 71 nursing staff
|
Table 4.1. Demographic data of study sample |
||||
|
Demographic Variables |
Variables Classes |
Frequency |
Percent % |
|
|
1- |
Male |
29 |
40.8 |
|
|
Gander |
Female |
42 |
59.2 |
|
|
Total |
71 |
100.0 |
||
|
2- |
Education level |
Middle school |
20 |
28.2 |
|
Diploma |
25 |
35.2 |
||
|
Bachelors |
19 |
26.8 |
||
|
Master |
3 |
4.2 |
||
|
PhD |
4 |
5.6 |
||
|
Total |
71 |
100.0 |
||
|
3- |
Years of experience |
less than 6 years |
24 |
33.8 |
|
6-10 years |
27 |
38.0 |
||
|
more than 10 years |
20 |
28.2 |
||
|
Total |
71 |
100.0 |
||
|
4- |
Housing environment |
City |
64 |
90.1 |
|
country side |
7 |
9.9 |
||
|
Total |
71 |
100.0 |
||
Table (4-1) Shows the demographic information of Health staff members who were included in the study. The majority (59.2%) of participants (Health staff members) related to Female gander, information on the education level, frequency Middle school is (20) and percentage (28.2%).
The diploma frequency was (25) and the percentage (35. 2%).was frequency the Bachelors (19) and percent (26.8%). Was frequency Master
(3) and percentage (4.2%). was frequency PhD (4) and percent (5.6%). Frequency the majority had 10-6 years of service (27) and percent (38.0%). In terms of housing environment, the majority from population a city (90.1%) percent of the sample and frequency is (64).
|
Questions |
N |
Mean Score |
Sd. |
Variance |
Knowledge |
|
Q1 |
71 |
0.58 |
0.280 |
0.078 |
Moderate |
|
Q2 |
71 |
0.36 |
0.300 |
0.090 |
Moderate |
|
Q3 |
71 |
0.92 |
0.335 |
0.112 |
Good |
|
Q4 |
71 |
0.79 |
0.318 |
0.101 |
Good |
|
Q5 |
71 |
0.92 |
0.476 |
0.227 |
Good |
|
Q6 |
71 |
0.96 |
0.318 |
0.101 |
Good |
|
Q7 |
71 |
0.83 |
0.377 |
0.142 |
Good |
|
Q8 |
71 |
0.96 |
0.350 |
0.123 |
Good |
|
Q9 |
71 |
0.92 |
0.364 |
0.133 |
Good |
|
Q10 |
71 |
0.71 |
0.390 |
0.152 |
Good |
|
Q11 |
71 |
0.71 |
0.390 |
0.152 |
Good |
|
Q12 |
71 |
0.83 |
0.364 |
0.133 |
Good |
|
Q13 |
71 |
0.88 |
0.390 |
0.152 |
Good |
|
Q14 |
71 |
0.92 |
0.300 |
0.090 |
Good |
|
Q15 |
71 |
0.88 |
0.300 |
0.090 |
Good |
|
Q16 |
71 |
0.50 |
0.350 |
0.123 |
Moderate |
|
Q17 |
71 |
0.54 |
0.438 |
0.192 |
Moderate |
|
Q18 |
71 |
0.33 |
0.377 |
0.142 |
Poor |
|
Q19 |
71 |
0.63 |
0.401 |
0.161 |
Moderate |
|
Q20 |
71 |
0.67 |
0.453 |
0.205 |
Moderate |
|
Q21 |
71 |
0.32 |
0.390 |
0.152 |
poor |
|
Q22 |
71 |
0.75 |
0.438 |
0.192 |
Good |
|
Q23 |
71 |
0.92 |
0.471 |
0.222 |
Good |
|
Q24 |
71 |
1.00 |
0.401 |
0.161 |
Good |
Table (4-2) shows the general information for the knowledge of the health employee about ERP who were included in the study and had good knowledge about the ERP system.
|
Table (4-6): Knowledge of health staff members towards the ERP system. |
||||
|
Knowledge |
Frequency |
Percent |
Valid Percent |
Cumulative Percent |
|
Poor |
1 |
1.4 |
1.4 |
100.0 |
|
Moderate |
15 |
21.1 |
21.1 |
98.6 |
|
Good |
55 |
77.5 |
77.5 |
77.5 |
|
Total |
71 |
100.0 |
100.0 |
|
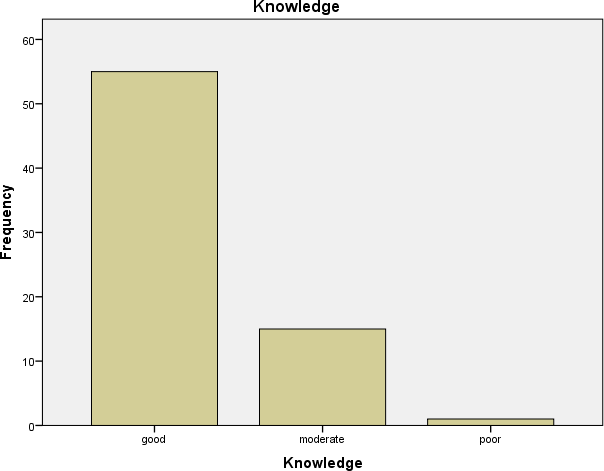
Table (4-3) Knowledge of health staff members towards the ERP system. Levels show the majority (good) percent was (77.5 %), and Knowledge Levels (Moderate) percent was (21.1 %), and Knowledge Levels (Poor) percent was (1.4%).
|
Table (4-7): Relationship between Demographic variables and health staff members about ERP |
|||
|
Demographic |
Chi-square |
P Value |
SIG |
|
1- Gander |
1.820 |
0.402 |
NS |
|
2-Education Level |
4.235 |
0.835 |
NS |
Figure 4.4.1 Bar chart Overall Knowledge of health staff members towards the ERP system (Poor = 1.4%, Moderate =21.1%, Good =77.5%)
|
3- Years of education |
1.935 |
0.748 |
NS |
|
4-Housing Environment |
2.25 |
0.323 |
NS |
P – value = probability level of≤ 0.05
This table shows the relationship between Knowledge of health staff members and information demographic about ERP. There is no significant no relationship between Knowledge of health staff members and information demographic about ERP.
Discussion of the Socio–Demographic Characteristics for the Study Sample
The total number of participants is 71 from the health staff, who have completed the surveys, and the majority of the participants were females (59.2) and they were the most participants from diploma graduates (35.2), and the percentage of middle school graduates was (28.2), and the percentage of bachelors was (26.8), the master was (4.2) and the doctorate (5.6) and they were the most participants city dweller.
Part II
Table 2 means (= 77.5 = true) where the ERP system records all
the data of the medical staff, workers, and the specialty of each individual with working hours is not acceptable in the study.” Siew Kien Sia, May Tang, Christina Soh, Wai Fong Boh ACM SIGMIS Database: the DATABASE for Advances in Information Systems [ 9 ] .
This paper explores ERP as an ambivalent technology of power, while another study agrees with it, Tina Blegind Jensen, Margunn Aanestad. Information systems management [10].
Through the ERP system it is possible to raise the efficiency of providing health services
An integrated supply chain management system: a case study in healthcare sector Dong soo Kim [11].
Conclusion :
According to the results of the current study, the researcher can State the following conclusions:
1- Most of the health personnel in hospitals and medical centers had a lack of knowledge regarding the impact of the ERP system
2 – Most of the study sample members (health staff) who participated in the study are diploma graduates, and they have (6-10) years of service.
3- The health staff members do not have sufficient knowledge in some aspects of the ERP system.
4 – There is no relationship between knowledge and demographic data ( Education level, years of experience, gender, housing environment)
5- For health personnel affiliates, it has no effect on knowledge of the ERP system.
6- The knowledge of the impact of the ERP system for the study sample was at a good level.
7- The study showed that the percentage of successful knowledge about the ERP system is 21.1% with weak knowledge, while 77.5% were with good knowledge.
Recommendations :
1. It was suggested to use this model as a yardstick to find out the impact of the ERP system.
2. Increasing the holding of intensive training courses under the supervision of a specialized cadre, and the establishment of continuous educational courses related to the ERP system.
3. Encouraging health personnel to update their information by participating in training courses and conferences inside and outside Iraq to improve their knowledge regarding the management of the enterprise resource planning system in hospitals and health care center
References :
- Al-Mashari, M., Al-Mudimigh, A., and Zairi, M. (2003) Enterprise resource planning: A taxonomy of critical factors, European Journal of Operational research, 146 352-364.
- KUMAR, KULDEEP, and JOS VAN HILLEGERSBERG. “ERP EXPERIENCES AND EVOLUTION.” Communications of the ACM, vol. 43, no. 4, Apr. 2000, p. 22. Gale Academic OneFile, link.gale.com/apps/doc/A61792746/AONE?u=anon~6ebdcbba&sid=go ogleScholar&xid=52d6800d. Accessed
- Hofmann,P, (2008). ERP is Dead, Long Live ERP, Internet Computing, IEEE, August 2008,124), pp. 84-88(
- Nah, F. F.-H., Lau, J. L.-S., & Kuang, J. (2001). Critical Factors for Successful Implementation of Enterprise Systems. Business Process Management Journal, 7, 285-296.
- Shehab, E., Sharp, M., Supramaniam, L., and Spedding, T. (2004) EntERPrise resource planning:
An integrative review’. Business Process Management Journal, 10 (4): 359-386
- Kolodner, R. M., S. P. Cohn, C. P. Friedman.(2008) Health information technology: Strategic initiatives, real progress. Health Affairs 27 w391–w395.
- Piontek, F., R. Kohli, P. Conlon, J. J. Ellis, J. Jablonski, N. Kini.(2010). Effects of an adverse-drugevent alert system on cost and quality outcomes in community hospitals. American J. Health-System Pharmacy 67(8) 613–620
8-Luay Abdulwahid Shihab , TECHNOLOGICAL TOOLS FOR DATA SECURITY IN THE TREATMENT OF DATA RELIABILITY IN BIG DATA ENVIRONMENTS, 10.14456/ITJEMAST.2020.175, International Transaction Journal of Engineering, Management, & Applied Sciences & Technologies .
9-Siew Kien Sia, May Tang, Christina Soh, Wai Fong Boh, 33 (1), 23-37, 2002
ACM SIGMIS Database: the DATABASE for Advances in Information Systems .
10. Valerie Botta-Genoulaz, Pierre-Alain Millet , 99 (1-2), 202-221, 2006, An investigation into the use of ERP systems in the service sector
International journal of production economics .
11. Igal M Shohet, Lorenzo Nobili , 65, 33-41, 2016 , Enterprise resource planning system for performance-based- maintenance of clinics Igal M Shohet, Lorenzo Nobili Automation in Construction .